Obesity is a growing worldwide epidemic, with an estimated 1.9 billion overweight people and 600 million obese adults.
Obesity is associated with significant morbidity and mortality due to its close association with cardiovascular disease and diabetes.
Even moderate weight loss may be associated with diabetes prevention, lower blood pressure, lower cholesterol and triglycerides, and other health benefits (1-3).
Alpha lipoic acid (ALA), also called thioctic acid, is a naturally occurring short-chain fatty acid that contains a thiol bond (4).
It is an important cofactor for energy production in mitochondria (5). ALA also exhibits properties as a powerful antioxidant and free radical scavenger (4, 6, 7). ALA is sold in many countries around the world as an over-the-counter dietary antioxidant supplement, alone or in combination with other antioxidants. In medicine, ALA is used to reduce the symptoms of diabetic polyneuropathy, and several clinical trials have established efficacy and an excellent safety profile in this patient population (8–13). In addition, ALA has a wide range of beneficial effects on obesity-related conditions such as insulin resistance, metabolic syndrome, and type II diabetes, including their complications such as vascular damage (5, 11).
Alpha Lipoic Acid (ALA) as a Weight Loss Supplement
Previous studies have shown the beneficial anti-obesity properties of ALA (14–16). In animal studies, ALA supplementation has been shown to reduce body weight and fat mass by reducing food intake and increasing energy expenditure, possibly also by inhibiting hypothalamic AMP-activated protein kinase (AMPK) activity (17–20).
However, in human studies with ALA supplementation, results were inconsistent. Some clinical trials have shown that ALA supplementation can help overweight and even obese people lose weight (15, 16), while other studies have not observed any effect of ALA on weight (21, 22). To more comprehensively evaluate the effects of ALA as a weight loss supplement. A systematic review and comprehensive meta-analysis of the available literature was recently conducted (27). A total of 11 eligible studies with 12 relevant treatments were identified for inclusion in this review. Of these studies, 8 reported results for weight and seven reported results for BMI. The studies in this meta-analysis were conducted in a variety of populations, including patients with diabetes mellitus (9, 21, 23), metabolic syndrome (24), rheumatoid arthritis (25), and nonalcoholic fatty liver disease (26). Three studies were designed as weight loss interventions and were conducted with overweight and obese people. The total number of participants in these studies was 534 in the ALC group and 413 in the placebo group.
The duration of the study ranged from 8 weeks to 52 weeks. ALA doses ranged from 300 mg/day to 1800 mg/day. Total weight loss was 1.27 kg greater with ALC treatment compared to the placebo group. A significant overall mean difference in body mass index (BMI) was also found; in the ALC group, BMI decreased by 0.40 kg/m2 more than in placebo.
There was no evidence of publication bias in the analyzes of changes in weight and BMI. Cumulative results in this meta-analysis showed significant reductions in body weight and BMI with ALA treatment compared with placebo, regardless of whether it was used for weight loss or other purposes. Meta-regression analysis showed that shorter duration of ALC intervention resulted in greater reduction in BMI than longer interventions.
Rates of adverse events and all-cause discontinuation were similar between ALC and placebo. In this analysis, intervention duration, but not ALA dose, was found to be significantly associated with reduction in BMI. The studies in this meta-analysis examined different doses of ALA (from 300 mg/day to 1800 mg/day) at different intervention durations (from 8 weeks to 52 weeks). One placebo-controlled study compared the effectiveness of different doses of ALA on body weight (16). Koh et al. (16) examined the effects of 1200 mg/day and 1800 mg/day ALA intervention on weight loss. They found that the higher dose of ALA resulted in significant reductions in weight and BMI throughout the study compared to placebo, and the lower dose resulted in significant weight reduction only in the first weeks of this study, however this effect was not sustained throughout the duration of the study. research. Based on these data, it can be argued that the effect of ALA on body weight is limited to the short term, especially when it is used in lower doses.
Thiolepta
The domestic drug thiolept (pharmacologically active substance - thioctic acid) is an endogenous antioxidant that inactivates free radicals and regulates the metabolism of lipids and carbohydrates. In clinical practice it is used for polyneuropathies: diabetic and alcoholic. In recent decades, the increase in the number of patients suffering from diabetes mellitus may not be noticed only by a person infinitely far from medicine. And if in 2000 this serious disease was indicated in the outpatient cards of 170 million inhabitants of the Earth, then in 2012 - already in 366 million. One of the late complications of diabetes mellitus is diabetic polyneuropathy, manifested by total damage to peripheral nerves. According to statistics, this pathology occurs in approximately 30% of diabetics. Intensive insulin treatment may reduce the risk of diabetic neuropathy, but it cannot be completely prevented. The drug whose effectiveness against diabetic neuropathy currently has the greatest evidence base is thioctic (alpha-lipoic) acid or thiolepta. The main role in the pathogenesis of diabetic neuropathy is played by oxidative stress, the biochemical “weapon” of which is free radicals. Preclinical studies of thioctic acid conducted on laboratory animals have demonstrated that this substance reduces the number of free radicals (including superoxide), reduces the intensity of the process of lipid peroxidation, stimulates endoneurial circulation, increases the rate of propagation of excitation along peripheral nerve fibers, and increases the utilization of glucose by myocardial cells , suppresses the development of cataracts, prevents glomerular kidney diseases. In clinical trials using thioctic acid in patients with diabetes mellitus, activation of blood flow in the microvasculature, suppression of lipid peroxidation, normalization of blood levels of nitric oxide and stress proteins (proteins synthesized under various physiological stresses), improvement of renal filtration, increase glucose utilization.
As for alcoholic polyneuropathy, according to modern concepts, it does not arise as a result of the disease, but at its very beginning, i.e., using medical terminology, “at the preclinical stage of alcohol abuse.” Polyneuropathy occupies a significant place in the clinical picture of the so-called. sluggish alcoholism, characterized by long-term, painful alcohol abuse (which is different, for example, from female alcoholism). In such cases, polyneuropathy is part of the pathogenesis of alcoholism and requires emergency treatment using thioctic acid drugs at any stage of the disease.
Thiolepta is available in tablets (at the moment, the dosage form of the drug in the form of a solution for intravenous infusion is not registered in the Russian Federation). When taken orally, it is quickly and completely absorbed from the gastrointestinal tract. The maximum concentration of the active substance in the blood is observed 40-60 minutes after taking the drug. Thiolept is prescribed 600 mg (1-2 tablets) 1 time per day. The drug should be taken in the morning, always on an empty stomach (simultaneous food intake reduces the rate of absorption), about half an hour before the first meal, with a sufficient amount of water. The duration of the medication course is determined by the doctor individually. Patients with diabetes mellitus during pharmacotherapy are advised to regularly monitor blood glucose levels (especially in the initial stage of treatment). In some cases, to avoid hypoglycemia, the dose of insulin or tableted hypoglycemic agent may be reduced. During treatment with thiolept, you should abstain from alcohol.
ALC in obstetrics and gynecology
A 2018 review analyzed the effects of ALA in gynecology and obstetrics, with a focus on neuropathic pain and antioxidant and anti-inflammatory effects.
Research data has demonstrated that ALA reduces oxidative stress and insulin resistance in women diagnosed with polycystic ovary syndrome (PCOS). A combination of N-acetylcysteine, alpha-lipoic acid and bromelain is used to prevent and treat endometriosis. A promising area of research is the use of ALC in patients with threatened miscarriage to improve the resorption of subchorionic hematoma. In addition, ALA can be used to prevent diabetic embryopathy and premature rupture of membranes caused by inflammation. The review findings noted that ALA can be used safely for the treatment of neuropathic pain and as dietary support during pregnancy (28).
ALA in the treatment of psychiatric and neurological disorders
Despite the existence of many preclinical studies, there is a lack of scientific data on the clinical use of ALA in diseases of the central nervous system. Therefore, in a systematic review last year (2019), the authors set out to review the literature regarding the use of ALA for the treatment of psychiatric and neurological conditions and identify what is missing from administering this antioxidant for this purpose (29). A total of 32 articles were included in the review. In psychiatric disorders, research on ALC in schizophrenia has advanced as ALC administration is associated with improvement in schizophrenia symptoms and antipsychotic side effects. In neurological disorders, ALA as a supplement has been effective in preventing the progression of Alzheimer's disease. In stroke, the use of a supplement containing 300 mg ALA presented important results, as there was a reversal of clinical parameters and oxidative imbalance in these patients. For other neurological conditions such as encephalopathy, multiple sclerosis, traumatic brain injury, mitochondrial disorders and migraine, the results are still preliminary.
Thioctic acid
Thioctic acid is a metabolic agent that regulates the metabolism of carbohydrates and fats. The instructions for use of this drug give only one indication - diabetic polyneuropathy. However, this is not a reason to downplay the importance of thioctic acid in clinical practice. This endogenous antioxidant has amazing abilities to scavenge harmful free radicals. Thioctic acid takes an active part in cellular metabolism, performing the function of a coenzyme in the chain of metabolic transformations of antitoxic substances that protect cells from free radicals. Thioctic acid potentiates the action of insulin, which is associated with the activation of the process of glucose utilization.
Diseases caused by endocrine and metabolic disorders have been in the area of special attention of doctors for more than a hundred years. At the end of the 80s of the last century, the concept of “insulin resistance syndrome” was first introduced into medicine, which united, in fact, insulin resistance, impaired glucose tolerance, increased levels of “bad” cholesterol, decreased levels of “good” cholesterol, and the presence of excess body weight and arterial hypertension. Insulin resistance syndrome has a similar name: metabolic syndrome. In contrast, clinicians have developed the basics of metabolic therapy aimed at maintaining or regenerating the cell and its basic physiological functions, which is a condition for the normal functioning of the entire organism as a whole. Metabolic therapy involves hormonal therapy, maintaining normal levels of chole- and ergocalciferol (vitamins D), as well as treatment with essential fatty acids, including alpha-lipoic or thioctic acid. In this regard, it is absolutely wrong to consider antioxidant therapy with thioctic acid only in the context of the treatment of diabetic neuropathy.
As you can see, this drug is also an indispensable component of metabolic therapy. Thioctic acid was originally called “vitamin N,” hinting at its importance for the nervous system. However, due to its chemical structure, this compound is not a vitamin. Without delving into the biochemical “wilds” with mention of dehydrogenase complexes and the Krebs cycle, we should note the pronounced antioxidant properties of thioctic acid, as well as its participation in the recycling of other antioxidants, for example, vitamin E, coenzyme Q10 and glutathione. Moreover: thioctic acid is the most effective of all antioxidants, while it is regrettable to note the current underestimation of its therapeutic value and the unreasonable narrowing of indications for use, which are limited, as already mentioned, only to diabetic neuropathy. Neuropathy is a degenerative-dystrophic degeneration of nervous tissue, leading to a disorder of the central, peripheral and autonomic nervous systems and desynchronization of the work of various organs and systems. All nervous tissue is affected, incl. and receptors. The pathogenesis of neuropathy is always associated with two processes: impaired energy metabolism and oxidative stress. Considering the “tropism” of the latter for nervous tissue, the clinician’s task includes not only a scrupulous diagnosis of signs of neuropathy, but also its active treatment with thioctic acid. Since treatment (or rather, even prevention) of neuropathy is most effective even before symptoms of the disease appear, it is necessary to start taking thioctic acid as early as possible.
Thioctic acid is available in tablets. A single dose of the drug is 600 mg. Given the synergism of thioctic acid with insulin, with the simultaneous use of these two drugs, an increase in the hypoglycemic effect of insulin and tablet hypoglycemic agents may be observed.
Effects of ALA on lipid profile and glycemic control
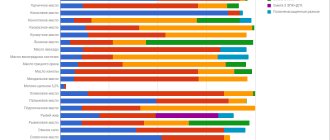
Randomized controlled trials (RCTs) have demonstrated that alpha lipoic acid (ALA) can alter lipid profiles. A 2019 meta-analysis of experimental data from 12 studies showed that serum levels of total cholesterol (TC) and low-density lipoprotein cholesterol (LDL) were significantly lower in patients given alpha-lipoic acid compared to controls. but no significant changes were found in high-density lipoprotein cholesterol (HDL-c) levels. The overall effect of ALA on serum triglyceride levels did not show any significant changes, but in a subgroup analysis based on health status (diabetic and nondiabetic), ALA reduced serum triglyceride levels in both diabetic and nondiabetic groups compared with control. This meta-analysis showed that ALA may have beneficial effects on lipid profiles, especially LDL and TC (30).
The results of another meta-analysis examining the effects of alpha lipoic acid (ALA) supplementation on both lipid profiles and glycemic control in patients with metabolic diseases showed that ALA supplementation significantly reduced fasting glucose, insulin, and insulin resistance homeostasis models. No negative effect was found on high-density lipoprotein (HDL) cholesterol levels (31).
conclusions
Results showed that alpha lipoic acid supplementation for 12 weeks improved insulin sensitivity, serum insulin levels, adiponectin and leptin levels without affecting BMI, waist circumference, liver enzymes, resistin and irisin.
Research data allows the use of dietary supplements with alpha-lipoic acid to reduce insulin resistance and normalize blood sugar levels in patients with diabetes, metabolic syndrome, obesity and NAFLD. Normalizing sugar levels helps reduce the risk of fatty liver degeneration in patients with obesity and diabetes.
Alpha Lipoic Acid Dosing
The dosage used by ALA varies widely and varies depending on the health condition and purpose of use.
Thus, for weight loss, people who are overweight or obese with an accompanying bouquet of metabolic disorders are recommended to take 600-1500 mg per day, divided into two doses, regardless of food intake. For the treatment and prevention of diabetes, 600-800 mg per day, divided into two doses, and for persons with diabetic neuropathy, the upper dose limit can reach up to 1800 mg. Healthy people taking ALA as an antioxidant may limit themselves to doses of 100-500 mg per day, regardless of meals, once a day.
However, in a study that tested whether ALA taken in conjunction with simple carbohydrates and creatine increased the uptake of the latter into muscle cells during the loading phase (20 g creatine per day) in healthy men, a dosage of 1000 mg per day ALA divided by several parts have been shown to be highly effective (32). Thus, healthy people can take a similar dosage in individual cases when massive creatine intake is planned.
Sources:
- Goldstein DJ. Beneficial health effects of modest weight loss. Int J Obes Relat Metab Disord. 1992;16:397–415.
- Knowler WC, Fowler SE, Hamman RF, et al. 10-year follow-up of diabetes incidence and weight loss in the Diabetes Prevention Program Outcomes Study. Lancet. 2009;374:1677–1686.
- Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346:393–403
- Evans JL, Goldfine ID. Alpha-lipoic acid: a multifunctional antioxidant that improves insulin sensitivity in patients with type 2 diabetes. Diabetes Technol Ther. 2000;2:401–413.
- Packer L, Kraemer K, Rimbach G. Molecular aspects of lipoic acid in the prevention of diabetes complications. Nutrition. 2001;17:888–895
- Bast A, Haenen GR. Lipoic acid: a multifunctional antioxidant. Biofactors. 2003;17:207–213.
- Deneke S.M. Thiol-based antioxidants. Curr Top Cell Regul. 2000;36:151–180.
- Ziegler D, Hanefeld M, Ruhnau KJ, et al. Treatment of symptomatic diabetic polyneuropathy with the antioxidant alpha-lipoic acid: a 7-month multicenter randomized controlled trial (ALADIN III Study). ALADIN III Study Group. Alpha-Lipoic Acid in Diabetic Neuropathy. Diabetes Care. 1999;22:1296–1301.
- Ziegler D, Schatz H, Conrad F, Gries FA, Ulrich H, Reichel G. Effects of treatment with the antioxidant alpha-lipoic acid on cardiac autonomic neuropathy in NIDDM patients. A 4-month randomized controlled multicenter trial (DEKAN Study). Deutsche Kardiale Autonome Neuropathie. Diabetes Care. 1997;20:369–373.
- Ametov AS, Barinov A, Dyck PJ, et al. The sensory symptoms of diabetic polyneuropathy are improved with alpha-lipoic acid: the SYDNEY trial. Diabetes Care. 2003;26:770–776.
- Ziegler D. Thioctic acid for patients with symptomatic diabetic polyneuropathy: a critical review. Treat Endocrinol. 2004;3:173–189.
- Ziegler D, Ametov A, Barinov A, et al. Oral treatment with alpha-lipoic acid improves symptomatic diabetic polyneuropathy: the SYDNEY 2 trial. Diabetes Care. 2006;29:2365–2370.
- Ziegler D, Nowak H, Kempler P, Vargha P, Low PA. Treatment of symptomatic diabetic polyneuropathy with the antioxidant alpha-lipoic acid: a meta-analysis. Diabet Med. 2004;21:114–121.
- Huerta AE, Navas-Carretero S, Prieto-Hontoria PL, Martinez JA, Moreno-Aliaga MJ. Effects of alpha-lipoic acid and eicosapentaenoic acid in overweight and obese women during weight loss. Obesity. 2015;23:313–321.
- Carbonelli MG, Di Renzo L, Bigioni M, Di Daniele N, De Lorenzo A, Fusco MA. Alpha-lipoic acid supplementation: a tool for obesity therapy? Curr Pharm Des. 2010;16:840–846.
- Koh EH, Lee WJ, Lee SA, et al. Effects of alpha-lipoic Acid on body weight in obese subjects. Am J Med. 2011;124:85.e1–8.
- Prieto-Hontoria PL, Perez-Matute P, Fernandez-Galilea M, Martinez JA, Moreno-Aliaga MJ. Effects of lipoic acid on AMPK and adiponectin in adipose tissue of low- and high-fat-fed rats. Eur J Nutr. 2013;52:779–787.
- Prieto-Hontoria PL, Perez-Matute P, Fernandez-Galilea M, Barber A, Martinez JA, Moreno-Aliaga MJ. Lipoic acid prevents body weight gain induced by a high fat diet in rats: effects on intestinal sugar transport. J Physiol Biochem. 2009;65:43–50.
- Prieto-Hontoria PL, Perez-Matute P, Fernandez-Galilea M, Martinez JA, Moreno-Aliaga MJ. Lipoic acid inhibits leptin secretion and Sp1 activity in adipocytes. Mol Nutr Food Res. 2011;55:1059–1069.
- Wang Y, Li X, Guo Y, Chan L, Guan X. alpha-Lipoic acid increases energy expenditure by enhancing adenosine monophosphate-activated protein kinase-peroxisome proliferator-activated receptor-gamma coactivator-1alpha signaling in the skeletal muscle of aged mice. Metabolism. 2010;59:967–976.
- Ansar H, Mazloom Z, Kazemi F, Hejazi N. Effect of alpha-lipoic acid on blood glucose, insulin resistance and glutathione peroxidase of type 2 diabetic patients. Saudi Med J 2011;32:584–588.
- McNeilly AM, Davison GW, Murphy MH, et al. Effect of alpha-lipoic acid and exercise training on cardiovascular disease risk in obesity with impaired glucose tolerance. Lipids Health Dis. 2011;10:217.
- Study of comparative effects of antioxidants on insulin sensitivity in type 2 diabetes mellitus. Udupa AS, Nahar PS, Shah SH, Kshirsagar MJ, Ghongane BB. J Clin Diagnosis Res. 2012 Nov; 6(9):1469-73
- The effect of lipoic acid and vitamin E therapies in individuals with the metabolic syndrome. Manning PJ, Sutherland WH, Williams SM, Walker RJ, Berry EA, De Jong SA, Ryalls AR. Nutr Metab Cardiovasc Dis. 2013 Jun; 23(6):543-9.
- Gargari BP, Kolahi S, Dehghan P, Khabbazi A, Mirtaheri E. Effects of Alpha-Lipoic Acid Supplementation on Clinical Status and Anthropometric Indices in Women with Rheumatoid Arthritis. Curr Top Nutraceut R. 2015; 13:33-40.
- Impact of combined therapy with alpha-lipoic and ursodeoxycolic acid on nonalcoholic fatty liver disease: double-blind, randomized clinical trial of efficacy and safety. Gianturco V, Troisi G, Bellomo A, Bernardini S, D'Ottavio E, Formosa V, Iacono CL, Verrusio W, Marigliano B, Marigliano V. Hepatol Int. 2013 Jun; 7(2):570-6.
- Alpha-Lipoic Acid (ALA) as a supplementation for weight loss: Results from a Meta-Analysis of Randomized Controlled Trials. Suat Kucukgoncu, Elton Zhou, Katherine B Lucas, and Cenk Tek.Obes Rev. May 2017; 18(5): 594–601.
- Alpha lipoic acid in obstetrics and gynecology. Di Tucci C, Di Feliciantonio M, Vena F, Capone C, Schiavi MC, Pietrangeli D, Muzii L, Benedetti Panici P. Gynecol Endocrinol. 2018 Sep;34(9):729-733.
- Alpha-lipoic acid in the treatment of psychiatric and neurological disorders: a systematic review. de Sousa CNS, da Silva Leite CMG, da Silva Medeiros I, Vasconcelos LC, Cabral LM, Patrocínio CFV, Patrocínio MLV, Mouaffak F, Kebir O, Macedo D, Patrocínio MCA, Vasconcelos SMM. Metab Brain Dis. 2019 Feb;34(1):39-52.
- Does alpha-lipoic acid affect lipid profile? A meta-analysis and systematic review on randomized controlled trials. Haghighatdoost F, Hariri M. Eur J Pharmacol. 2021 Mar 15;847:1-10.
- The effects of alpha-lipoic acid supplementation on glucose control and lipid profiles among patients with metabolic diseases: A systematic review and meta-analysis of randomized controlled trials. Akbari M, Ostadmohammadi V, Lankarani KB, Tabrizi R, Kolahdooz F, Khatibi SR, Asemi Z. Metabolism. 2018 Oct;87:56-69.
- Effect of alpha-lipoic acid combined with creatine monohydrate on human skeletal muscle creatine and phosphagen concentration. Burke DG, Chilibeck PD, Parise G, Tarnopolsky MA, Candow DG. Int J Sport Nutr Exerc Metab. 2003 Sep;13(3):294-302.
About alpha lipoic acid without cuts
No matter where in the world I speak about treating complications of diabetes, I always get a question about the same substance. Do you think we are talking about insulin? No! About glucose? Also no. We are talking about alpha-lipoic acid, also known as thioctic acid, as well as the well-known drugs Berlition, Thioctacid, Thiogamma and other commercial names. According to many people, this magical substrate should prevent the development of chronic complications of the disease, and first of all, “protect your legs from diabetes” (this is a quote from one of my patients, as you understand).
This is the main idea of this note: only achieving your target glucose level will protect you and your organs from the complications of diabetes. This has been known since the first publication of the results of the DCCT study, which, by the way, you can read about here. Still, it was a revolutionary and very large-scale event, which for the first time showed that complications of diabetes are a consequence of decompensation, and not a manifestation of the disease.
The target blood glucose level, and not any substances, even with beautiful names, is our most important assistant in the fight for a life without diabetes complications. Was I strict enough? Because I would like this to sound very strict. Because it's important.
Now let's look at where this belief in the magic of alpha lipoic acid comes from. The theoretical part is really very beautiful, believe me, a big fan of biochemistry. So that you don't have to open the textbook, I'll remind you of a few points.
- In order to function, we need energy. From a biochemical point of view, energy exists in the body in the form of ATP molecules.
- ATP molecules are formed in the cell through reactions called the Krebs cycle.
- Let's remember chemistry: in every reaction, in addition to the directly reacting substances, additional substances also participate; they are called enzymes. Enzymes themselves do not react, but they are extremely necessary - without them the process will not work.
- Enzymes often require coenzymes to function. In most cases, they are derivatives of vitamins or their metabolites and are needed to activate the enzyme.
Why is it important to know and understand - even without details - some biochemical processes?
Because, firstly, there is a lot of biochemistry in diabetology - the concepts of “glycolysis”, “gluconeogenesis”, “glycogen” and the like are worth it. And secondly, because this is the only way to dilute the information that is broadcast to us by manufacturers of various kinds of drugs to increase the significance of a particular substance.
For me, a person for whom logical explanations are very important, the most understandable way to study the story about alpha-lipoic acid is the biochemical one. I promise it will be as simple as possible.
Why do we need alpha lipoic acid?
- Alpha lipoic acid is a coenzyme necessary for the oxidative decarboxylation reaction of pyruvate. In human terms, it is involved in the process of energy formation in cells.
- As a coenzyme, lipoic acid is also involved in the enzymes of the alpha-ketoglutarate dehydrogenase reaction. These are participants in the Krebs cycle, in which, as you already read above, energy is produced in the form of ATP molecules.
Alpha-lipoic acid is produced in small but sufficient quantities in our bodies, as well as in red meat, liver, kidneys, potatoes, and yeast. Its normal level is 1-25 ng/ml. It turns out that very little of this substance is needed for the normal functioning of the body. You can get it from many sources. Where does the story about at least 600 mg intravenous administration for 10 days come from?
And yes, the idea that alpha-lipoic acid is a powerful antioxidant has a right to exist, but what do diabetes complications have to do with it? I answer: from the assumption (a good word, I really like it in this context) that alpha-lipoic acid is a super antioxidant, and people with diabetes really, really need it. And the more of these antioxidants there are (600, 1200, 1800 mg per day - who is more?), the better.
In order to save your time, I will not present the results of clinical studies of the properties of magic acid, which have now been completed. I will only voice a conclusion: none of the studies talk about alpha-lipic acid as a means that will help prevent the development of complications of diabetes in humans . In general, it will not “protect your legs from diabetes.” Sadness.
Some reduction in the severity of pain symptoms - yes, some improvement in sensory symptoms (sensitivity) - yes. There are even limited data on successful attempts to treat autonomic neuropathy in the form of high heart rate variability, as well as sexual function - oh yes.
In general, an interesting story came out about a vitamin-like substance that, of course, will not harm you. But, alas, it will not work as a means that “protects against diabetes” in conditions of non-target blood sugar levels. Unfortunately.